Diabetic Foot: Why a Vascular Surgeon is Your Feet’s Best Friend
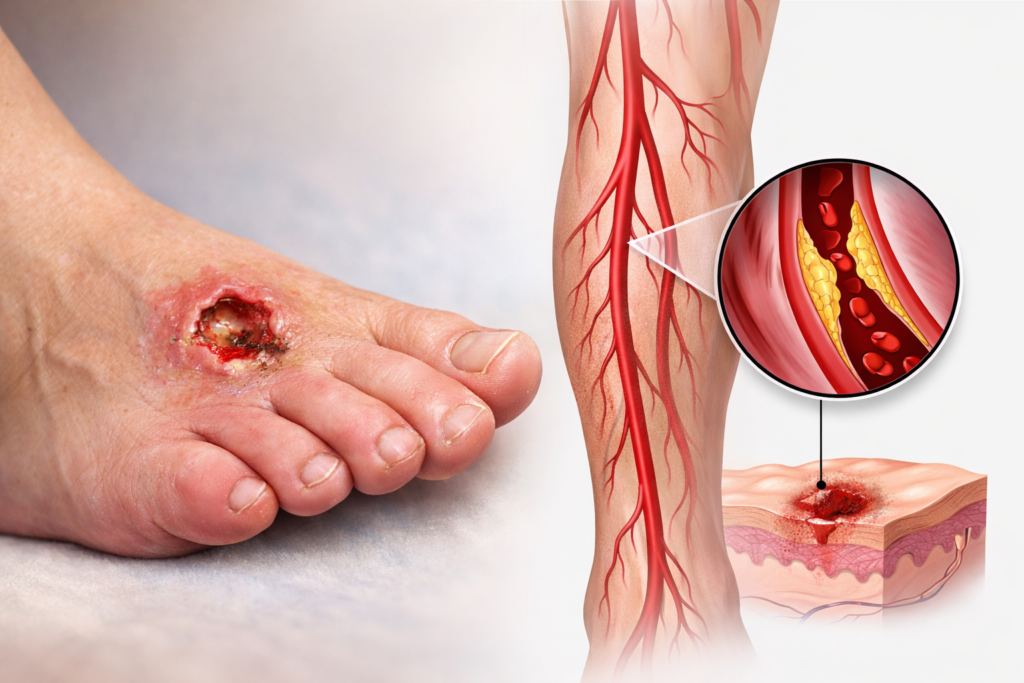
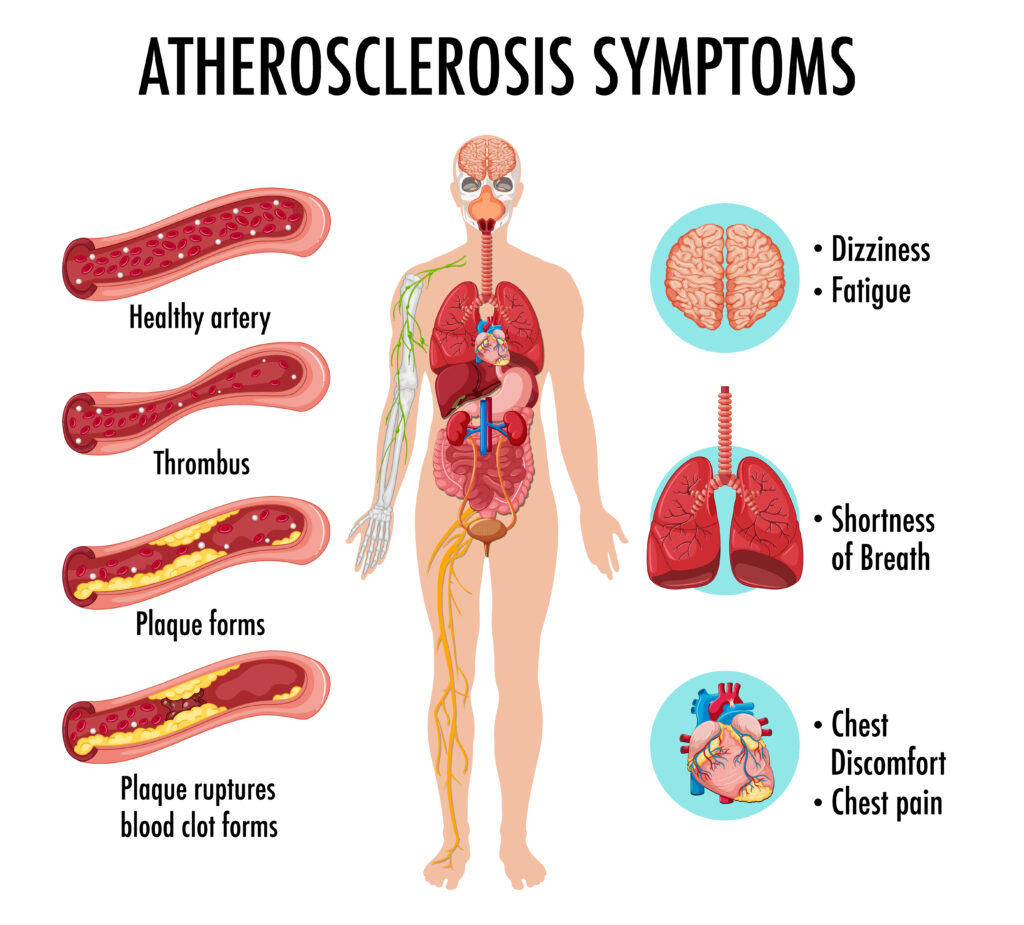
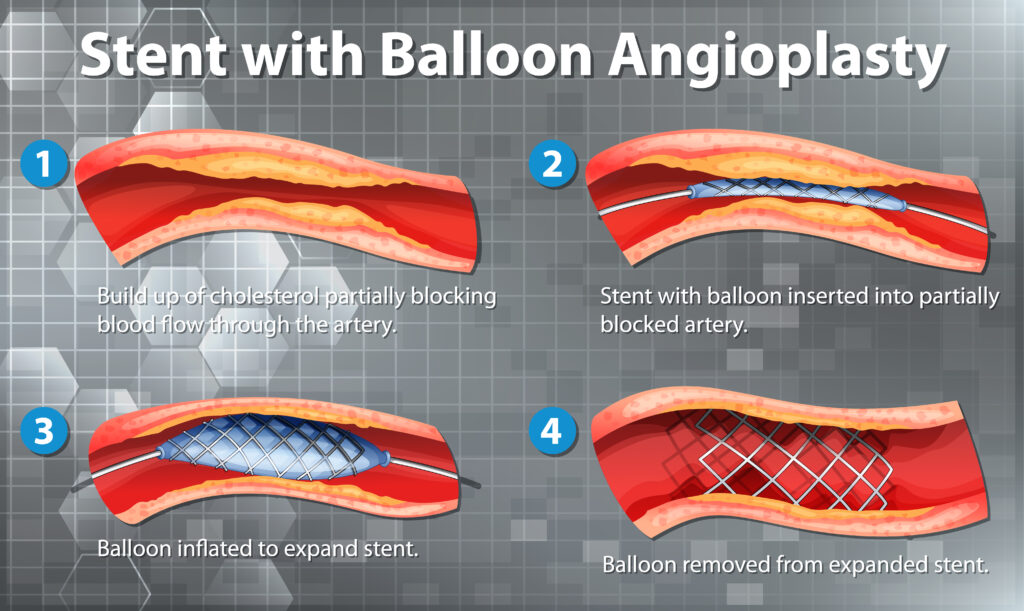
Diabetic Foot: Why a Vascular Surgeon is Your Feet’s Best Friend If you have diabetes, you’ve likely been told to check your feet every day. But if a complication arises—like a wound that won’t heal, a change in skin color, or a persistent ache—you might wonder who the right specialist is. While podiatrists and wound care experts are vital, the Vascular Surgeon plays a unique and critical role in saving the diabetic foot. Here is why a vascular specialist is the “anchor” of your foot health team. It’s All About the “Fuel Lines” Diabetes is a disease that affects the blood vessels. Over time, high blood sugar can cause the arteries in your legs to narrow or clog—a condition called Peripheral Artery Disease (PAD). Think of your arteries as the “fuel lines” carrying oxygen and nutrients to your feet. If those lines are blocked, your skin cannot repair itself, and your immune system cannot reach a wound to fight off infection. A vascular surgeon is the only specialist trained to physically reopen those fuel lines using advanced techniques like: Angioplasty and Stenting: Using tiny balloons to widen narrowed arteries from the inside. Bypass Surgery: Creating a new path for blood to flow around a blockage. Preventing the “Silent” Threat Many diabetic patients suffer from neuropathy (nerve damage), meaning they can’t feel a pebble in their shoe or a developing blister. Because you can’t feel the pain, a small nick can quickly turn into a deep ulcer. A vascular surgeon doesn’t just treat the wound; we evaluate the entire circulatory system. We use specialized tests to measure exactly how much oxygen is reaching your toes. By catching poor circulation early—even before a wound appears—we can prevent the tissue death that leads to amputation. The Goal: Limb Preservation The ultimate goal of a vascular surgeon is Limb Salvage. We look at the “big picture” of your health: Restoring Flow: Ensuring the foot has enough blood to heal. Infection Control: Working with other doctors to stop the spread of bacteria. Healing: Providing the vascular foundation that allows wound care treatments to actually work. When to See Us You should ask for a vascular evaluation if you have diabetes and notice: A sore or ulcer that hasn’t improved in two weeks. Your feet feel cold to the touch or look pale/blue. Pain in your calves while walking that goes away with rest. Rest pain (pain in your feet that keeps you up at night). Remember: In the world of diabetic foot care, “Time is Tissue.” Addressing circulation issues early is the most effective way to stay mobile and keep your feet healthy.
Diabetic Foot: Why a Vascular Surgeon is Your Feet’s Best Friend Read More »